3.1.0.1 Primary diagnoses
- Eating disorders
- Anovulatory uterine bleeding
- Some primary care patients admitted for Gen Peds issues
Parents, family members, or other involved adults should NOT be present during the HEEADSSS interview. Addressing this and the need for confidentiality at the beginning of the visit is important. Before asking adults to leave the room, always ask whether they have any concerns to express or questions to ask and assure them of further interaction once the confidential interview is over. Sometimes having a confidential moment with the adult can also be very informative to the patient’s care.
Consider starting your HEEADSSS assessment by asking about the patient’s strengths. A simple question such as “What are your greatest strengths” can go a long way in rapport building and eliciting motivations to engage in healthy behavior change.
Bold (green) = essential questions
Italics (blue) = as time permits
Plain text (red) = optional or when the situation requires
| Screeners | When to use | |
|---|---|---|
| Depression | PHQ-2, PHQ-A = PHQ-9 modified for adolescents, PSC-17 (up to age 15) | - Routine Child Health Maintenance visits - Visits for mood follow-up - When you’re concerned about depression and/or suicidality in your patient |
| Anxiety | PSC-17 (up to age 15), GAD-7, SCARED | - Routine Child Health Maintenance visits - Visits for mood follow-up - When you’re concerned that anxiety is a problem for your patient |
| Substance Use | S2BI, CRAFFT, BSTAD | - Routine Child Health Maintenance visits - F/u after visits in the ED for acute intoxication - When you’re concerned that substance use is a problem for your patient |
| Notes | Access | |
|---|---|---|
| Ella (ulipristal acetate) | - Most effective EC pill to prevent pregnancy up to 5 days after unprotected sex - Do NOT give if starting any form of hormonal contraception (ulipristal binds the progesterone receptors and blocks the hormone’s effects) |
- Rx ONLY - Safe to call in a prescription w/o pregnancy test or seeing patient |
| Plan B One-Step (levonorgestrel 1.5mg) | - Works to prevent pregnancy for the first 3 days after unprotected sex - Works less well in patients who are overweight or obese - Discuss with your preceptor if you should recommend a double dose for your overweight patients |
- Sold (at cost $$, w/o Rx) to anyone of any age at most pharmacies, though access is still difficult for adolescents. Much cheaper w/ Rx. - Safe to call in a prescription w/o pregnancy test or seeing patient |
| Copper IUD (Paragard) | - Most effective form of EC (>99%), effective up to 7 days after unprotected sex - Can provide up to 12 years of highly effective contraception after placement |
Must be placed in a clinic setting by a trained provider |
For more information on emergency contraception (EC), please see the following resources: Bedsider, reproductiveaccess.org, Mass.gov EC site
For more information on contraceptive methods, minor consent laws, as well as medical eligibility criteria and selected practice recommendations, please see the following resources: Center for Young Women’s Health, Bedsider, Reproductive Access, CDC MEC, CDC SPR, Guttmacher Institute
** NOTE: Treatments change frequently! Check the CDC Treatment Guidelines or download the “CDC STD Tx Guide” app.
| Signs & Symptoms | Diagnosis | Management | |
|---|---|---|---|
| Physiologic (leukorrhea) | - Clear, white, or grey discharge; no offensive odor - No burning or itching |
- pH < 4.5 - Wet mount: epithelial cells w/ no or few leukocytes |
Reassurance |
| Candida vaginitis (“yeast infection”) | - Odorless curd-like white clumpy discharge - Intense burning and pruritus |
- pH < 4.5 - KOH: No fish odor, +budding yeast and pseudohyphae, +WBC - Vaginitis Panel via vaginal swab (tests for BV, Candida Vaginitis, Trich) |
- Fluconazole 150 mg PO (single dose) - Miconazole or clotrimazole intravaginal cream |
| Trichomoniasis | - Malodorous, frothy, yellow-green or cream colored discharge - Pruritus, dysuria |
- pH > 4.5 - KOH: Fish odor may be present - Wet mount: WBC and pear shaped organism w/ motile flagella - Vaginitis Panel via vaginal swab (tests for BV, Candida Vaginitis, Trich) - NAAT dirty urine collection |
- Metronidazole 2g PO (single dose) or 500mg PO BID for 7 days Partner: treat and refrain from intercourse for 7 days |
| Bacterial vaginosis (BV) | - Malodorous, increased mild grey-white discharge - Mild or absent pruritis or burning |
- pH > 4.5 - KOH: +Fish odor - Wet mount: >20% clue cells-epithelial cells covered w/ gram negative rods - Vaginitis Panel via vaginal swab (tests for BV, Candida Vaginitis, Trich) |
- Metronidazole 500mg PO BID for 7 days, OR - Metronidazole gel 0.75% one applicator (5g) intravaginally daily for 5 days Partner: treat if recurrent infection |
| Gonorrhea (GC) | - Majority asymptomatic - Grey-white cervical discharge |
GC/CT NAAT vaginal swab or dirty urine | - Ceftriaxone 250mg IM + azithromycin 1g PO (co-tx chlamydia and covers resistant gonorrhea) - Refrain from intercourse x7 days Partner: Evaluate and treat contacts w/i prior 60 days |
| Chlamydia (CT) | - Majority asymptomatic - Yellowish vaginal discharge |
GC/CT NAAT vaginal swab or dirty urine | - Azithromycin 1g PO x1 - If allergic to azithro, can do doxycycline 100mg PO BID x7 days - Refrain from intercourse x7 days Partner: Evaluate and treat contacts w/i prior 60 days |
| Retained tampon | Malodorous discharge | History and PE | Remove tampon |
| Allergic vaginitis | Local pain, vaginal erythema | History of exposure to deodorant spray, scented tampons, etc. | Cessation of sensitizing agent |
| PEP = Post-Exposure Prophylaxis | PrEP = Pre-Exposure Prophylaxis | |
|---|---|---|
| EBG | Sexual Assault EBG | PrEP EBG |
| What is it? | Always a 3 drug regimen: - Preferred regimen (tablets only): Truvada (tenofovir and emtricitabine) + Raltegravir - Alternative regimen (if unable to swallow pills): Zidovudine + Lamivudine, + Raltegravir (chewtab) OR Lopinavir/Ritonavir (liquid) |
Daily Truvada (tenofovir-emtricitabine) |
| Who’s it for? | Consider PEP if the following three statements apply to the patient: - Isolated anal, vaginal, percutaneous or oral exposure to possibly or definitely HIV infected blood or semen - Exposure occurred within 72 hours of presentation - Patient/family will consent to treatment and agree to follow-up |
HIV neg Adolescents/Adults weighing >35 kg and meeting one of the following indications: - Men who have sex with men - Person who injects drugs - Heterosexual men and women at substantial risk of acquiring HIV infection (any sex partner w/ HIV or HIV risk factors, hx of bacterial STI, hx injecting drugs, used non-occupational PEP, survival/transactional sex, been in drug tx program, interest in trying to conceive w/ a discordant partner) |
| Signs & Symptoms | Diagnosis | Treatment | |
|---|---|---|---|
| Genital herpes | Grouped vesicles, painful shallow ulcers, tender inguinal adenopathy | - Tzanck smear and viral culture - Antigen testing to determine HSV1 vs. HSV2 can give more information about recurrence prognosis |
First episode: - Acyclovir 400mg TID x5-10 days, OR - Valacyclovir 1g BID x7-10 days Recurrent episodes: - Acyclovir 400mg TID x5 days, OR - Valacyclovir 500 mg BID x3 days Daily suppressive (maintenance) therapy: - Acyclovir 400 PO BID - Valacyclovir 500mg-1g PO daily |
| Genital warts | - Single or multiple soft fleshy papillary or sessile painless growths around genitals - No inguinal lymphadenopathy |
- Initial: clinical presentation - Final: Pap test revealing typical cytologic changes |
Goal: remove exophytic warts; exclude cervical dysplasia before treatment Medication (not in preg): - Podophylin 0.5% gel BID x3 days then off x4 days, and repeat up to 4 times; OR - Imiquimod 5% cream 3x/wk on alternate days until resolution (<16 wks) Prevention: Gardasil 9-valent vaccine (HPV(6, 11, + 7 others) |
| Syphilis | - Primary: Indurated, well defined, usually single painless ulcer “chancre” - Secondary: weeks to months later; systemic infection w/ rash, fever, HA, malaise, anorexia, adenopathy - Latent → Leads to Tertiary in 25%: CNS, cardiac manifestations; gummatous lesions |
- Initial: FTA-ABS, MHA-TP, dark-field microscopy or DFA test of exudate or tissue - Final: VDRL, RPR (reverse sequence screening @ BCH) - False seronegatives seen in first 3 months; presumptive tx recommended |
Primary and Secondary: - Benzathine Penicillin G: 2.4 mil U IM x1 dose - Doxycycline 100mg BID x14 days for allergy/preg Latent: infected but no sx - Benzathine Penicillin G: 2.4 mil U IM qweekly x3 wks Partner: evaluate if contact w/i 3 mo for primary, 6 mo for secondary, 1 year for latent |
| Chancroid | - Multiple, ragged, painful, non-indurated ulcers - Painful suppurative inguinal adenopathy |
- Initial: clinical presentation, neg syphilis and HSV - Final: culture of haemophilus ducreyi |
- Azithromycin 1g PO x1 dose - Ceftriaxone 250 mg IM x1 dose - Ciprofloxacin 500 mg BID x3 days - Erythromycin 500 mg TID x7 days Partner: evaluate and treat contacts w/i 10 days of symptoms |
** NOTE: Epididymitis is the male equivalent of female PID!
Pelvic Inflammatory Disease EBG
Infection of upper genital tract (cervix, uterus, fallopian tubes, ovaries)
N. gonorrhea, C. trachomatis or other anaerobic organisms
Pelvic pain, dyspareunia, vaginal discharge, fever, menstrual irregularities associated w/ lower abdominal tenderness, adnexal tenderness, and/or cervical motion tenderness
Uterine, adnexal, or cervical motion tenderness +/- LQ or RUQ tenderness
Partner: Evaluation and treatment of contacts w/i prior 60 days recommended. Refrain from intercourse in the meantime
Heavy/Irregular Menstrual Bleeding EBG
Abnormalities in the frequency, duration, volume, and/or timing of menstrual bleeding
Anovulatory bleeding (most common cause in adolescents), pregnancy (must rule out even w/o report of sexual activity), coagulopathy, recent start/stop of contraception
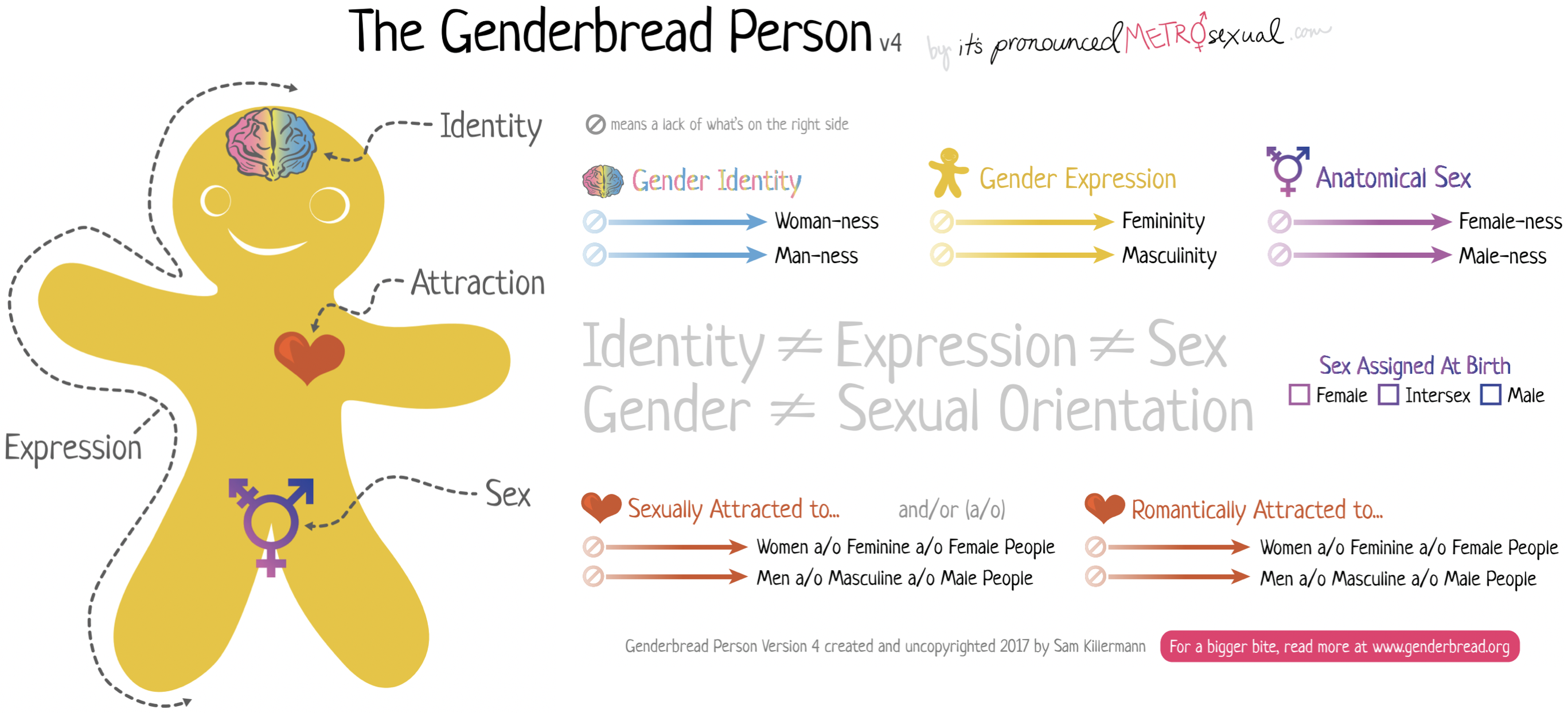
One of our roles as providers of gender diverse youth is to combat the adverse experiences and risk factors for developing mental health disorders by building safe communities for our patients and adopting a gender affirming approach to care.
Weight loss, abdominal pain, bloating, constipation, cold intolerance, lanugo, fatigue, weakness, delayed puberty
Low body temp, bradycardia, low blood pressure, orthostasis, lanugo, dry skin and hair, scalp hair thinning, scaphoid abdomen, palpable stool, breast atrophy, hypoestrogenized vaginal mucosa
See AN, PLUS: Esophagitis and cavities
See AN, PLUS: Calluses on fingers, cavities, and tooth decay
See AN, PLUS: Purge precautions (no bathroom privileges (use bedside commode), room searches)
ARFID protocol and PowerPlan
See AN, PLUS: Fear of choking or vomiting, limited range of preferred foods becomes narrower over time, will only eat certain textures of food, etc.
Goldenring JM, Rosen DS. Getting into adolescent heads: an essential update. Contemp Pediatr. 2004;21:64.↩︎
Mays A. IUD Counseling: What’s choice got to do with it? In: Optimizing IUD Delivery for Adolescents and Young Adults. Coles MS, Mays A, editors. New York, NY: Springer; 2019.↩︎
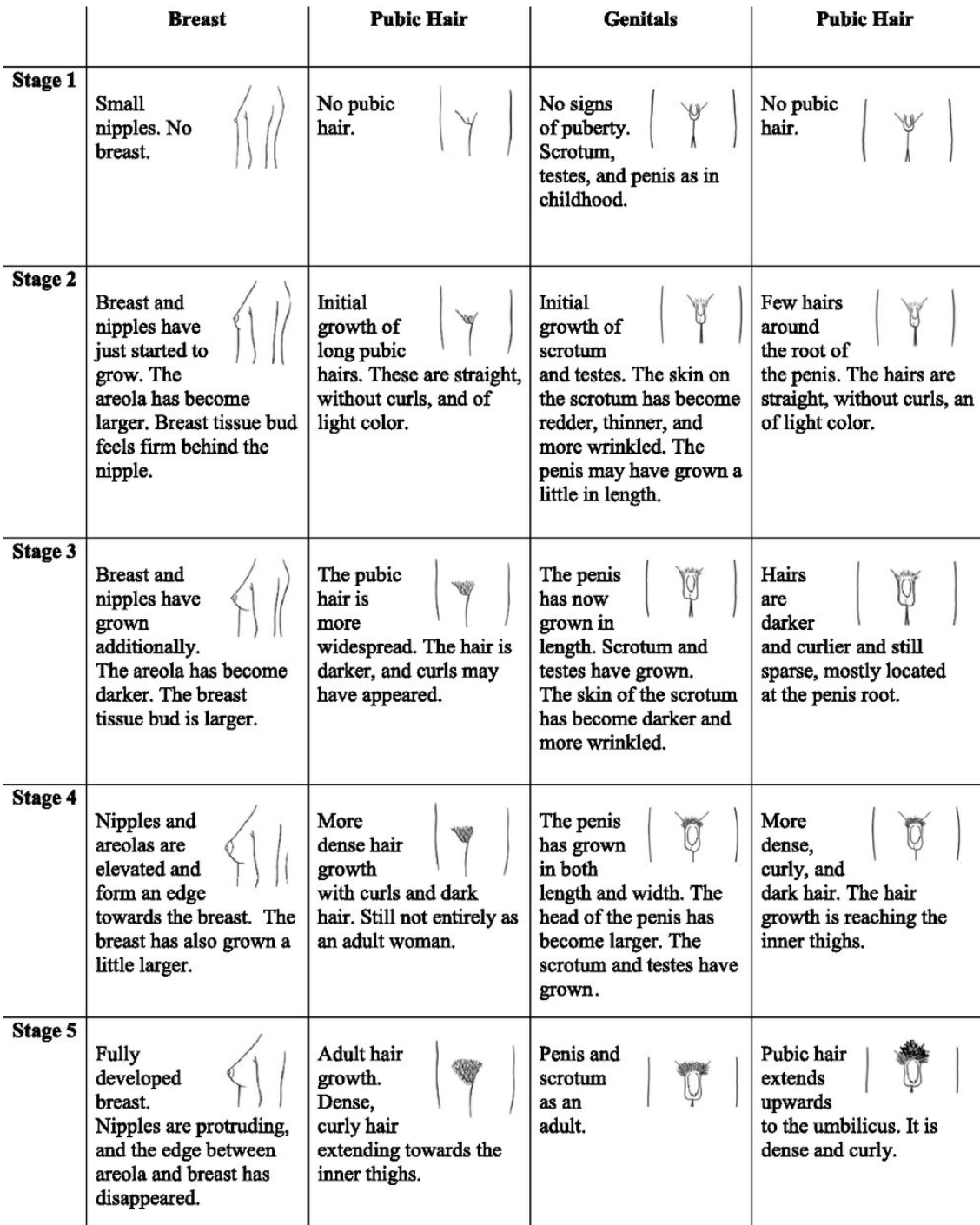
Morris NM, Udry JR. Validation of a self-administered instrument to assess stage of adolescent development. J Youth Adolesc. 1980;9(3):271–280pmid:24318082.↩︎
Welt, C. Etiology, diagnosis, and treatment of secondary amenorrhea. www.uptodate.com. Literature review current through: Feb 2019. | This topic last updated: Mar 21, 2018.↩︎